Medicare Access and Chip Reauthorization Act (MACRA) Proposed Rule, MIPS, APM’s and Advanced Care Information
The Centers for Medicare and Medicaid Services (CMS) released its proposed 962 page rule for the Medicare Access and CHIP Reauthorization Act (MACRA) of that links Medicare provider payments to quality patient care. The proposed regulation is the first major step taken by the government to implement the 2015 MACRA.
The proposed rule creates a “Quality Payment Program” to replace old reporting programs. There two tracks, the first called the Merit-based Incentive Payment System (MIPS) consolidates components of the Physician Quality Reporting System (PQRS), the Value-based Payment Modifier (VM), and the Medicare Electronic Health Record (EHR) Incentive Program. A second track involves alternative payment models (APM). Because of the high bar set to qualify for the APM track, CMS projects that only 30,000 to 90,000 clinicians will be in the APM track. An estimated 687,000 to 746,000 physicians will be in MIPS.
The program will begin grading physicians in 2017 for changes in their payments starting 2019.
Merit-based Incentive Payment System (MIPS)
CMS anticipates that most Medicare clinicians will initially participate in the Quality Payment Program through MIPS. CMS’s is hopeful that the proposed rule would improve the relevancy and depth Medicare’s quality-based payments and increase clinician flexibility by allowing clinicians to choose measures and activities appropriate to the type of care they provide.
CMS believes that MIPS allows Medicare clinicians to be paid for providing high value care through success in four performance categories: Quality, Advancing Care Information, Clinical Practice Improvement Activities, and Cost.
-
Quality (50 percent of total score in 2017): For this category, clinicians would choose to report six measures from among a list of options that accommodate differences among specialties and practices.
-
Advancing Care Information – Formerly Meaningful Use (25 percent of total score in 2017): For this category, clinicians would choose to report customizable measures that reflect how they use technology in their day-to-day practice, with a particular emphasis on interoperability and information exchange. Unlike the existing reporting program, this category would not require all-or-nothing EHR measurement or redundant quality reporting.
-
Clinical Practice Improvement Activities (15 percent of total score in 2017): This category would reward clinical practice improvements, such as activities focused on care coordination, beneficiary engagement, and patient safety. Clinicians may select activities that match their practices’ goals from a list of more than 90 options.
-
Cost (10 percent of total score in 2017): For this category, the score would be based on Medicare claims, meaning no reporting requirements for clinicians. This category would use 40 episode-specific measures to account for differences among specialties.
Winners and Losers
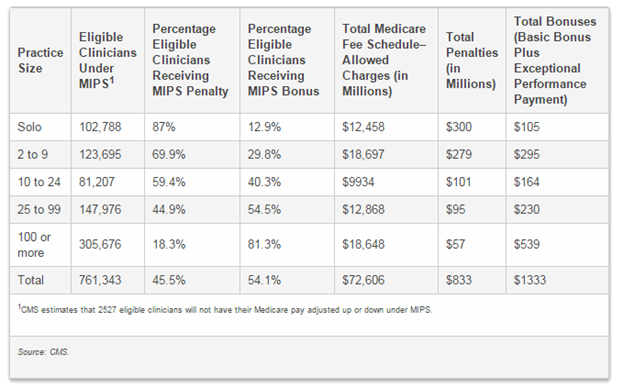
CMS estimates that there will be significant winners and losers under MIPS with some classes of eligible providers receiving positive adjustments and some negative the range is staggering between 79% positive adjustments and 98% negative adjustments or penalties. CMS estimates that small and solo practices will be especially hard hit by penalties under MIPS with 87% of solo practices estimated to be penalized.
Estimated MIPS Adjustments
| Winners |
Positive Adjustment |
| Cardiology |
62.1% |
| Endocrinology |
67.3% |
| Emergency Medicine |
64.0% |
| Colorectal Surgeons |
59.7% |
| Family Practice |
59.5% |
| Gastroenterology |
61.5% |
| Nurse Practitioners |
62.0% |
| Pediatrics |
79.3% |
| Physician Assistant |
67.1% |
| Rheumatology |
67.7% |
| Thoracic Cardiac Surgery |
61.8% |
| Urology |
59.2% |
|
Negative Adjustment |
|
| Losers | |
| Chiropractors |
-98.4% |
| Dentists |
-68.9% |
| General Practice |
-69.4% |
| Optometry |
-79.7% |
| Podiatry |
-78.0% |
| Plastic Surgery |
-65.4% |
| Psychiatry |
-68.8% |
| Physical Medicine |
-57.9% |
Source CMS MACRA Proposed Rule, Table 63, pages 672-675
Changes to Meaningful Use
One of the biggest changes as a result of the regulation could be the sunset of the Meaningful Use program through the “advancing care information” proposal (25 percent of the MIPS score). Under this new program, physicians will be allowed to select the measures that reflect how they use EHR technology and what suits their practices. CMS will no longer require all-or-nothing EHR measurement or quality reporting. The number of measures will be reduced from 18 to a new all-time low of 11. Reporting of clinical decision support and computerized physician order entry will no longer be required. EPs only have to report to a single public health immunization registry. Some physicians will also be exempt from reporting when EHR technology is less applicable.
The rule also emphasizes interoperability, information exchange and security measures and requires patients to have access to their health information through of APIs.
The program would align with the Office of the National Coordinator for Health IT’s 2015 certification criteria. These changes apply to professionals in the Medicare Meaningful Use program; however, penalties for the program do not end until the end of 2018 (performance year 2016). But the proposed rules will not impact professionals in the Medicaid program or hospitals
Quality
Quality is 50 percent of the score and clinicians pick six measures from a range of options that accommodate different specialties and practice settings. The final 10 percent of the MIPS score in the first year is related to cost. The score would be based on Medicare claims and uses 40 episode-specific measures to account for differences among specialties. There will also be significant credit given under MIPS for participation in an ACO or Patient Centered Medical Home,
Clinical Practice Improvement Activities and CME
Starting in 2017 (with payments in 2019 being impacted), the proposal outlines the four components of MIPS. MIPS is based on a 100 point score with clinical practice improvement activities (CPIA) representing 15 percent of the score. This is an area where CME should play an important role in helping CMS achieve its quality measure objectives. The proposed rule leaves great discretion to the Secretary of HHS to define what will be included in these activities. As stated in the rule’s preamble: “Clinical Practice Improvement Activity (CPIA) means an activity that relevant eligible clinician organizations and other relevant stakeholders identify as improving clinical practice or care delivery and that the Secretary determines, when effectively executed, is likely to result in improved outcomes.”
According to the statute, any CPIA measure must be “relevant to an existing CPIA subcategory (or a proposed new subcategory)” as defined in §414.1365. Unfortunately, those subcategories do not currently include a specific reference to medical education or a related area. The subcategories outlined in the proposed rule include: (1) expanded practice access; (2) population management; (3) care coordination; (4) beneficiary engagement; (5) patient safety and practice assessment; (6) participation in an APM; (7) achieving health equity; (8) emergency preparedness and response; and (9) integrated behavioral and mental health.
However, the language defining CPIA, and authority granted to the Secretary of HHS as proposed, offers an opportunity for advocates of CME to argue that CME should be included in the measurement category. In §414.1355, CMS proposes that CPIA be defined on an annual basis and must meet certain criteria – much of which aligns closely with the goals of CME. While CME may not be directly relevant to an existing CPIA subcategory, it does improve beneficiary outcomes, leads to practice improvement, can be performed by providers of all types, is feasible to implement, can be validated by CMS, and is evidence-based.
Even if no changes were made to the proposed rule, a strong case can be made before CMS as to why CME should be included in the CPIA score. But it would still be wise of CMS to expand the subcategories outlined in §414.1365 to include medical education through comments in the final rule.
Alternative Payment Models
CMS set a high bar on requirements for APM track. Under the agency’s criteria for payment models to be eligible for the APM track—which CMS calls “Advanced APMs”—the Bundled Payments for Care Improvement (BPCI) Initiative, the Comprehensive Care for Joint Replacement (CJR) Model, and Track 1 of the Medicare Shared Savings Program (MSSP) all will not qualify as APM’s under the proposed rule. However, MSSP Tracks 2 and 3, Next Generation, and Pioneer—which all require downside risk—will qualify.
The proposed rule confirms that only Part B (traditional) Medicare payments will count toward the Advanced APM threshold. Payments from Medicare Advantage plans can count toward the “Other Payer” threshold beginning in 2021, but only if those payments are made through models that meet Advanced APM requirements. The rule does not address whether CMS will allow Track 1 ACOs to switch MSSP tracks mid-participation agreement to join an Advanced APM.
To be considered an “Advanced APM”, the model must meet three criteria: The APM must require participants to use certified EHR technology; the APM must provide for payment for covered professional services based on quality measures comparable to those in the quality performance category under MIPS; and the APM must either require that participating APM entities bear risk for monetary losses of a more than nominal amount under the APM, or be a Medical Home Model expanded under section 115A(c) of the Act.
Another critical area of the APM section involves the definitions that will be associated with “financial risk criterion” and in excess of “nominal amount”. CMS writes that financial risk for monetary losses under an APM must be tied to performance under the model and cannot be solely indirect losses related to financial investments made by the APM entity. Nominal is intended to be “minimal in magnitude” but not “a mere formality.” The agency describes as an example that the law was not intended to consider one dollar of risk to be more than nominal.
To address risk of a nominal amount, CMS measures three specific dimensions: (a) marginal risk, which is a common component of risk arrangements—particularly those that involve shared savings—that refers to the percentage of the amount by which actual expenditures exceed expected expenditures for which an APM entity would be liable under the APM; (b) minimum loss rate (MLR), which is a percentage by which actual expenditures may exceed expected expenditures without triggering financial risk; and (c) total potential risk, which refers to the maximum potential payment for which an APM entity could be liable under the APM. CMS also proposes that for a APM to meet the nominal amount standard the specific level of marginal risk must be at least 30 percent of losses in excess of expected expenditures, and a minimum loss rate, to the extent applicable, must be no greater than 4 percent of expected expenditures, and total potential risk must be at least 4 percent of expected expenditures.
Discussion
Welcome news is the elimination of the all or nothing criteria of the meaningful use program. The exclusion of most ACO’s under Medicare shared shavings is probably the most controversial part of the proposed rule as health systems have invested millions in the current Medicare shared savings program. That CMS is estimating that 87% of solo practitioners will be paying a penalty will also not be well received. Under MIPS CMS is estimating that non MD providers with the exception of nurse practitioners and physician assistants fare the worst including Chiropractors, Podiatrists and Dentists. Overall the proposed rule creates and opportunity for input from stakeholders on the final version of MACRA. We will include further analysis of this rule in the days ahead.
Comments are due on June 27, 2016 To Submit Comments